What Doctors Wish Patients Knew About Prediabetes
What Doctors Wish Patients Knew About Prediabetes
Your doctor has about ten minutes with you. In that window they have to read your labs, ask about your meds, address whatever you came in for, and then squeeze in the sentence: “Your blood sugar is creeping up — you’re in the prediabetes range.”
There is so much they don’t get to say. The nuance, the reassurance, the warnings, the honest truth about what actually moves the needle — all of it gets compressed into a referral pamphlet you’ll probably leave in the car.

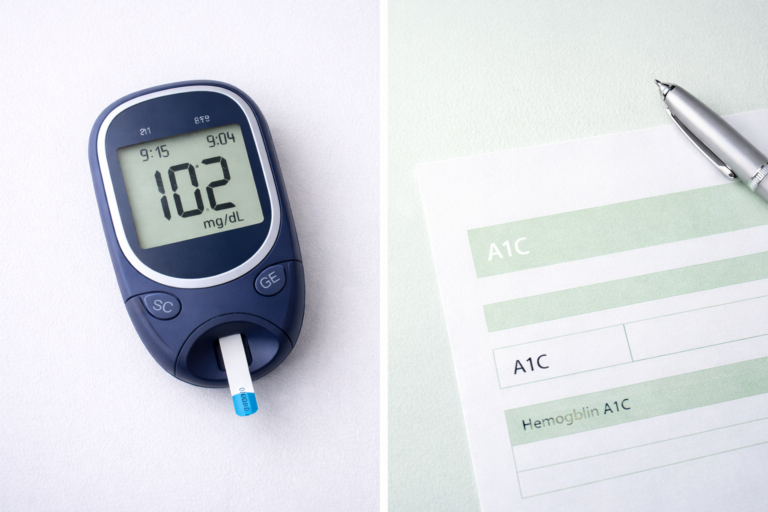
I’m Sarah Mitchell. When my own A1C came back at 6.1%, I got the rushed version too. It took me months of reading studies and talking to clinicians to fill in the blanks — and by then I’d brought my A1C down to 5.4%. This article is the longer conversation: the things doctors genuinely wish their prediabetes patients understood.
Quick Answer: Doctors wish prediabetes patients knew that the condition is a warning, not a sentence — it’s frequently reversible. They want you to understand that small, consistent habits compound, that sleep and stress matter as much as diet, that you don’t have to lose dramatic weight to improve, that supplements support but never replace lifestyle change, and above all that ignoring it is the single biggest mistake. Caught early and acted on, most people can return to a normal A1C below 5.7%.
Why This List Matters
According to the CDC, roughly 98 million U.S. adults — about 1 in 3 — have prediabetes, and more than 80% don’t know it. If you have a diagnosis, you’re already in the informed minority.
But knowing the label isn’t the same as knowing what to do with it. The gap between “your blood sugar is high” and “here’s exactly how I turned it around” is where most people get stuck and silently progress toward type 2 diabetes.
So let’s close that gap. Here are the ten things clinicians most often wish they’d had time to tell you.
1. Prediabetes Is a Warning, Not a Diagnosis of Failure
The word “pre” matters. You are before the line, not over it. Doctors see prediabetes as one of the few moments in medicine where the body hands you a clear, early heads-up while there’s still abundant room to change course.
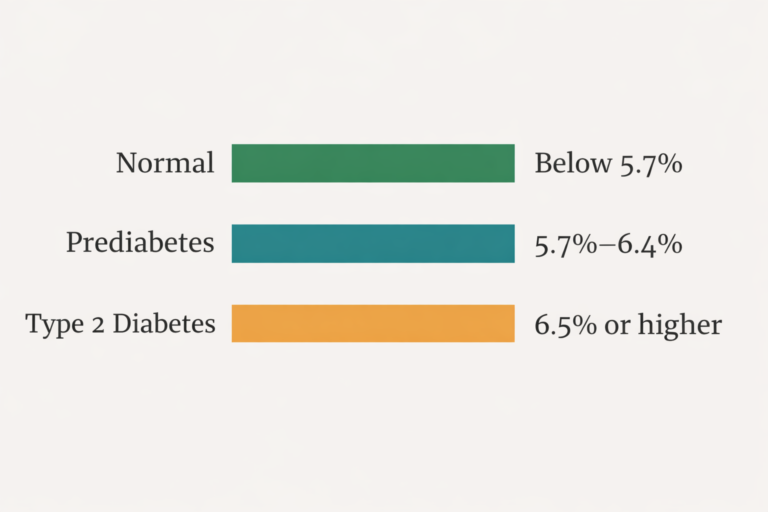
An A1C in the 5.7%–6.4% range means your average blood sugar has been elevated, but your body is still producing and responding to insulin well enough to recover. That window is precious — and it doesn’t stay open forever.
For the full picture of where your number sits and how the bands work, read our prediabetes A1C levels explained guide.
2. Yes, It Is Often Reversible
This is the single most reassuring thing doctors wish patients believed sooner. Prediabetes is not a one-way street. Many people return to a normal A1C through diet, movement, and lifestyle change.
What surprises patients most: 2026 research highlighted by ScienceDaily suggests prediabetes can be reversed even without significant weight loss — improvements in how your muscles use glucose can happen on their own as you move more and eat better.
We unpack the evidence in can prediabetes be reversed naturally and lay out a structured path in our reverse prediabetes naturally in 30 days plan.
3. You Don’t Need Dramatic Weight Loss to Improve
Patients often hear “prediabetes” and assume they’re being told to lose 40 pounds. Doctors wish you knew the truth is gentler: even modest changes in body composition and activity meaningfully lower blood sugar.
Insulin sensitivity improves with movement and muscle use, not just with the number on the scale. A daily walk after meals can blunt glucose spikes immediately — long before any weight changes.
See the science in does walking after meals lower blood sugar and the bigger reframe in you don’t need to lose weight to reverse prediabetes.
4. Small Changes Compound — That’s the Whole Strategy
Doctors don’t expect you to overhaul your life overnight. In fact, they’d rather you didn’t, because dramatic plans collapse. What works is the boring math of small, repeated choices.
Swap the soda for sparkling water. Walk after dinner. Add protein and fiber to breakfast. Each habit is small, but stacked together over months, they’re exactly what moved my A1C from 6.1% to 5.4%.
The compounding effect is why a 7-day prediabetes meal plan beats a crash diet, and why better breakfast ideas for prediabetes have outsized impact — breakfast sets your glucose tone for the whole day.
5. Sleep and Stress Are Blood-Sugar Issues — Not Just “Wellness”
This one shocks patients. You can eat perfectly and still see a stubborn A1C if you’re sleeping five hours a night or living in chronic stress.
Poor sleep raises cortisol and insulin resistance. Stress hormones tell your liver to dump glucose into your bloodstream — useful if you’re being chased, counterproductive if you’re just answering emails at midnight. Doctors wish patients treated sleep as a core part of the treatment, not an afterthought.
We go deep on this in how stress and poor sleep are making your prediabetes worse.
6. The Glycemic Quality of Your Food Matters More Than Calories
Counting calories alone misses the point. Two breakfasts with identical calories can produce wildly different blood-sugar responses. A bowl of cereal and juice spikes you; eggs with avocado and berries barely moves the line.
Doctors wish patients focused on what the food does to glucose, not just how much energy it holds. Fiber, protein, and fat slow sugar absorption; refined carbs accelerate it.
| Higher-Spike Choice | Steadier Swap | Why It Helps |
|---|---|---|
| Sugary cereal + juice | Eggs + avocado + berries | Protein and fat slow glucose release |
| White toast | Whole-grain or sourdough | More fiber, lower glycemic load |
| Flavored yogurt | Plain Greek yogurt + nuts | Cuts added sugar, adds protein |
| Instant oatmeal packet | Steel-cut oats + cinnamon | Slower digestion, gentler curve |
Learn the framework in glycemic index of breakfast foods and the full eating guide in what to eat (and avoid) with prediabetes.
7. Supplements Can Support You — But They Are Not Magic
Doctors get asked about berberine, cinnamon, and chromium constantly. Here’s the honest version they wish landed: certain supplements have real, measured effects, but none of them replace the foundation of diet, movement, and sleep.
The evidence is genuinely interesting. A 2021 meta-analysis found berberine lowers fasting glucose comparably to some oral medications, with low hypoglycemia risk. A 2019 meta-analysis of 16 trials (1,098 people) found cinnamon modestly reduces fasting glucose and insulin resistance. And a large 2020 cohort of 43,559 people linked higher vitamin D status to lower diabetes risk in prediabetics.
You can browse the wider evidence on PubMed and review the major options in our best supplements for prediabetes to lower A1C pillar. If you’re comparing specific formulas, our best blood sugar supplements of 2026 roundup breaks down what’s actually in them.
The doctor’s caveat stands: think of supplements as a tailwind, never the engine. And always tell your physician what you’re taking, especially if you’re on other medications.
8. Don’t Wait for Symptoms — Prediabetes Is Usually Silent
One of the most dangerous beliefs doctors fight is “I feel fine, so it can’t be serious.” Prediabetes typically has no symptoms. That’s precisely why more than 80% of people who have it don’t know.
By the time symptoms like excessive thirst, fatigue, or blurred vision appear, the condition has often progressed. Doctors wish patients acted on the number, not on how they feel. The lab result is the symptom.
If you were recently diagnosed, our just diagnosed with prediabetes 30-day plan gives you immediate, low-overwhelm steps.
9. Your Follow-Up Appointment Is Not Optional
Doctors wish patients understood that prediabetes management is a feedback loop. You change habits, you re-test, you adjust. Skipping the recheck means flying blind.
Most clinicians recommend re-testing your A1C every 3 to 6 months while you’re actively working on it. That cadence catches progress (motivating!) or backsliding (correctable) early. The NIDDK emphasizes that regular monitoring is central to prevention.
Come to those visits prepared. Our list of 6 questions to ask your doctor about prediabetes turns a rushed appointment into a useful one.
10. You Have More Control Than You Think
Maybe the most important thing of all. Patients often leave a prediabetes diagnosis feeling that diabetes is now inevitable — a slow countdown they can’t stop. Doctors wish they could erase that fear.
The data says otherwise. Prediabetes is one of the most modifiable conditions in all of medicine. The choices you make at breakfast, after dinner, and at bedtime genuinely change your trajectory.
That’s not toxic positivity — it’s what the research shows, and it’s what I lived. The path to lowering your A1C naturally is real, and it starts with believing you can walk it.
What Doctors Wish You’d Stop Doing
The flip side is just as useful. A few habits clinicians quietly wish their prediabetes patients would drop:
- Googling worst-case scenarios at 2 a.m. Anxiety raises blood sugar; it doesn’t lower it.
- Trying to fix everything in one week. Sustainable beats heroic. Pick one or two changes and build.
- Treating supplements as a license to keep eating badly. They can’t out-run a high-sugar diet.
- Hiding the diagnosis out of shame. Telling your household helps; support changes outcomes.
- Ignoring the recheck because you “feel fine.” Remember — it’s silent.
Key Takeaways
- Prediabetes is a warning, not a verdict — and it’s frequently reversible.
- Small habits compound. Walking after meals, better breakfasts, and steadier carbs add up over months.
- Sleep and stress are blood-sugar tools, not optional extras.
- You don’t need dramatic weight loss to meaningfully improve insulin sensitivity.
- Supplements support, never replace, lifestyle change — and your doctor should know what you take.
- It’s silent. Act on the number, not on symptoms, and never skip the follow-up A1C.
Frequently Asked Questions
Is prediabetes serious if I feel completely fine?
Yes. Prediabetes is almost always symptomless, which is exactly why more than 80% of people who have it don’t know. Feeling fine is normal and tells you nothing about your blood sugar. Doctors want you to treat the lab number itself as the signal to act, because acting early is when reversal is most achievable.
How quickly can I reverse prediabetes?
Many people see meaningful A1C improvement within 3 to 6 months of consistent diet, movement, and sleep changes, since A1C reflects your average blood sugar over the prior 2–3 months. Some return to a normal range (below 5.7%) within a few months. Your starting number, consistency, and other health factors all influence the timeline.
Do I have to lose a lot of weight to fix my blood sugar?
No. While weight loss can help, 2026 research suggests prediabetes can improve even without significant weight loss. Movement, muscle use, and better food quality improve how your body handles glucose independently of the scale. A daily post-meal walk lowers spikes immediately, long before any weight changes appear.
Will supplements like berberine or cinnamon reverse my prediabetes on their own?
No. Berberine and cinnamon have real, evidence-backed effects on fasting glucose, but they support lifestyle change rather than replace it. Doctors view them as a tailwind, not the engine. Use them alongside diet, movement, and sleep, and always tell your physician what you’re taking, especially if you’re on other medications.
How often should I recheck my A1C?
Most clinicians recommend re-testing every 3 to 6 months while you’re actively working to lower it. This cadence lets you catch progress or backsliding early and adjust your plan. Skipping follow-up testing means you’re managing a silent condition with no feedback, which doctors strongly discourage.
Can stress and poor sleep really raise my blood sugar?
Yes, significantly. Short sleep and chronic stress raise cortisol and insulin resistance, prompting your liver to release more glucose. You can eat well and still see a stubborn A1C if sleep and stress aren’t addressed. That’s why doctors treat them as core parts of prediabetes management, not optional wellness extras.
The Bottom Line
If your doctor had an extra twenty minutes, this is roughly the conversation you’d have. Prediabetes is your body asking for a course correction while there’s still plenty of road ahead.
You don’t need perfection. You need a few consistent habits, regular check-ins, and the belief — backed by real evidence — that you can change your trajectory. I did it, going from 6.1% to 5.4%, and the clinicians who treat this every day genuinely wish more patients knew it’s possible.
Start with one change this week. Then build from there.
For the complete roadmap, our complete guide to prediabetes pulls every piece of this together in one place.
Editor’s Recommendation
Quality supplementation is one tool doctors acknowledge — GlucoTrust is our top-rated blood sugar supplement.
15 research-referenced ingredients · 180-day money-back guarantee · GMP-certified