
The Complete Guide to Prediabetes: What It Means and How to Reverse It Naturally
Prediabetes means your blood sugar is elevated — higher than normal, but not yet high enough for a type 2 diabetes diagnosis. It affects 98 million American adults, and most of them have no idea they have it. The condition produces no obvious symptoms, but it does produce one clear biological opportunity: at this stage, the process is still reversible.
The Diabetes Prevention Program, the largest prediabetes study ever conducted, proved that lifestyle changes reduce the risk of progressing to type 2 diabetes by 58% over three years. That result has been replicated in Finland, China, India, and across multiple healthcare systems worldwide. Reversal is not a fringe claim — it is the consensus finding of clinical medicine.
This guide covers everything you need to understand your prediabetes diagnosis, read your lab results accurately, and take the specific steps that the evidence says work.
What This Guide Covers
- What prediabetes actually is — the biology in plain language
- How to read your A1C, fasting glucose, and OGTT numbers
- Why most people with prediabetes have no symptoms
- The 5 proven strategies to reverse it naturally
- What questions to ask your doctor at your next visit
- How long reversal takes — realistic expectations
The statistics and diagnostic criteria in this guide are drawn from the CDC prediabetes overview, which estimates 98 million U.S. adults have prediabetes, and the NIDDK clinical definition of prediabetes.
About this guide: This page explains what prediabetes is, how it is diagnosed, and what your lab numbers mean. For the specific action protocol on how to lower A1C and reverse the condition naturally, see the dedicated guide: How to Reverse Prediabetes Naturally: The 90-Day Protocol.
What Is Prediabetes?
Prediabetes is a metabolic state in which blood glucose levels are chronically elevated above normal, but not yet at the threshold for a type 2 diabetes diagnosis. The underlying mechanism is insulin resistance: your body produces insulin, but your muscle, fat, and liver cells respond to it less efficiently than they should, so blood glucose remains elevated after eating and does not clear quickly.
Over time, insulin resistance causes the pancreatic beta cells — the cells that produce insulin — to work harder to compensate. In many people, this compensatory capacity eventually fails, and blood sugar rises into the diabetic range. That progression is not inevitable. It is preventable, and in many cases reversible, with specific lifestyle interventions.
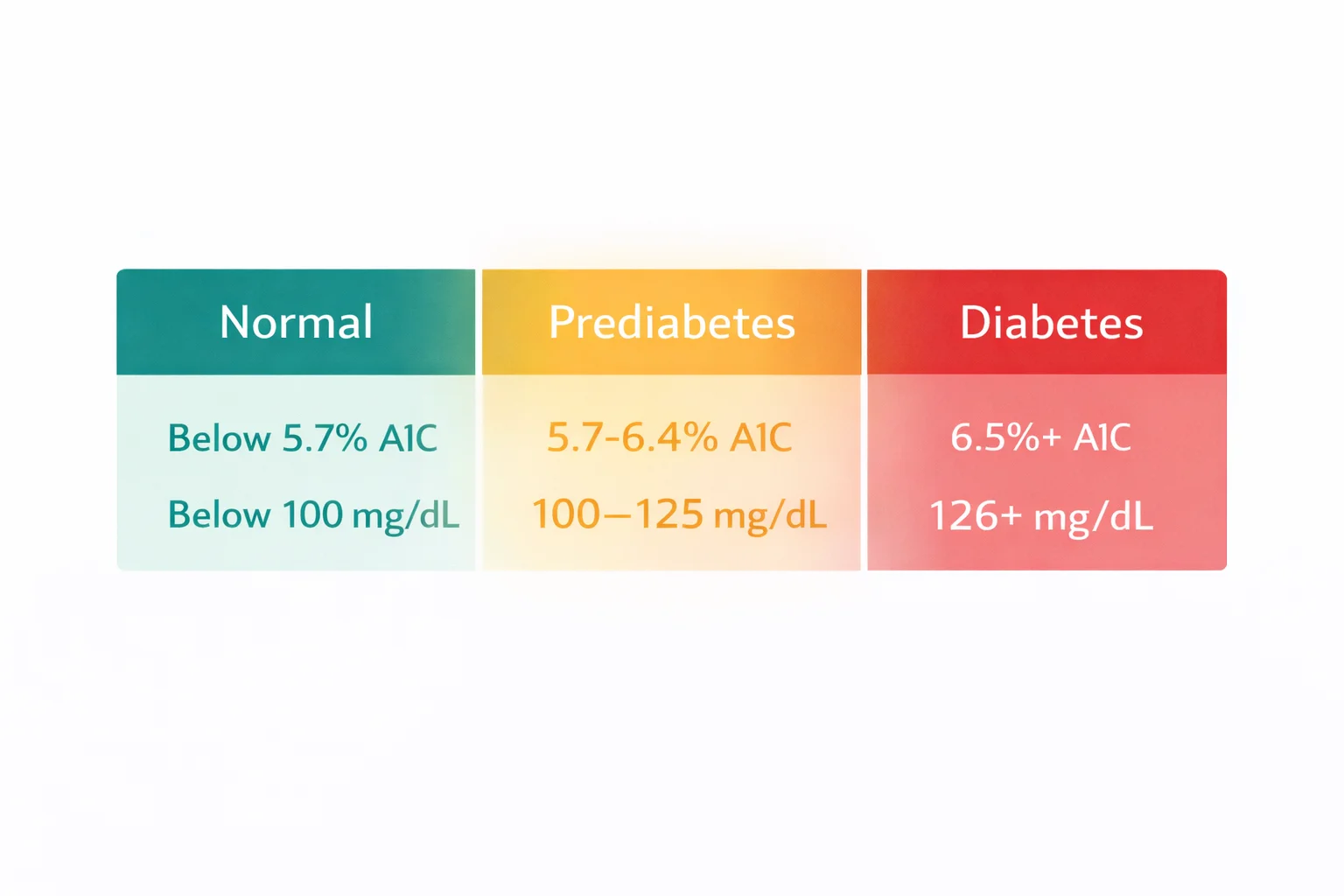
According to the American Diabetes Association’s 2025 Standards of Care, prediabetes is diagnosed when any of the following criteria are met:
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| A1C (HbA1c) | Below 5.7% | 5.7% – 6.4% | 6.5% or above |
| Fasting Plasma Glucose (FPG) | Below 100 mg/dL | 100 – 125 mg/dL | 126 mg/dL or above |
| 2-Hour OGTT | Below 140 mg/dL | 140 – 199 mg/dL | 200 mg/dL or above |
For a detailed explanation of what each test measures and how to interpret your specific result: read our complete guide to prediabetes A1C levels.
Why Prediabetes Has No Symptoms
Most people diagnosed with prediabetes feel completely normal. That is not a coincidence — it is a feature of how insulin resistance develops. The process happens gradually over years, and in the early stages the pancreas compensates by producing extra insulin. Blood sugar stays near normal ranges because the body is working harder to keep it there, not because anything is actually fine at the cellular level.
By the time you receive a prediabetes diagnosis from a blood test, insulin resistance has typically been present for several years. The absence of symptoms is precisely why the CDC estimates that 80% of people with prediabetes are unaware they have it. Diagnosis requires a blood test — it cannot be detected by how you feel.
Some people do notice certain patterns that are associated with insulin resistance — fatigue after meals, difficulty losing weight despite effort, hunger returning quickly after eating, skin darkening in folds (acanthosis nigricans) — but none of these are reliable diagnostic indicators. Only lab work confirms the diagnosis.
What Causes Prediabetes?
Insulin resistance — the root cause of prediabetes — is driven by a combination of genetic predisposition and lifestyle factors. The lifestyle factors are the ones you can change:
- Excess visceral fat — Fat stored around abdominal organs secretes inflammatory compounds that directly impair insulin receptor signaling. Visceral fat is more metabolically active than subcutaneous fat and is strongly associated with insulin resistance even at normal body weight.
- Physical inactivity — Skeletal muscle is the primary site of glucose disposal after meals. Inactive muscle develops reduced GLUT4 transporter expression, meaning glucose cannot enter cells efficiently regardless of insulin levels.
- Refined carbohydrate and ultra-processed food intake — High-glycemic foods produce rapid glucose spikes that require large insulin responses, over time contributing to receptor desensitization.
- Chronic sleep deprivation — Even one week of sleeping less than 6 hours per night measurably reduces insulin sensitivity in healthy adults. Cortisol elevation from poor sleep directly promotes hepatic glucose production.
- Chronic psychological stress — Sustained cortisol and adrenaline elevation trigger gluconeogenesis (glucose production by the liver) independent of food intake.
Understanding which of these factors is most relevant to your situation helps prioritize where to focus. For most people, a combination of movement, dietary improvement, and sleep quality produces the best outcome. For a detailed look at how sleep and stress specifically affect prediabetes: read our guide to stress, sleep, and prediabetes.
Can Prediabetes Be Reversed?
Yes. Reversal — defined as returning A1C and fasting glucose to the normal range and maintaining them there — is achievable for most people with prediabetes through lifestyle changes. This is the central finding of the Diabetes Prevention Program (DPP), a landmark randomized controlled trial funded by the NIH and published in the New England Journal of Medicine in 2002.
The DPP enrolled 3,234 adults with prediabetes and randomly assigned them to one of three conditions: intensive lifestyle intervention, metformin, or placebo. The lifestyle intervention group reduced progression to type 2 diabetes by 58% over three years, compared to 31% for metformin. The lifestyle intervention was the more effective treatment — at any age. Among participants over 60, the lifestyle group reduced progression by 71%.
The Finnish Diabetes Prevention Study (Tuomilehto et al., NEJM 2001) reached the same conclusion in a European population, with a 58% risk reduction from lifestyle intervention. These findings have since been replicated across dozens of healthcare systems and population groups worldwide.
Reversal does not require extreme interventions. The DPP lifestyle group achieved their result with: a 7% reduction in body weight (about 15 pounds for a 200-pound person), 150 minutes of moderate-intensity exercise per week, and modest dietary improvement focused on fat and calorie reduction. The bar is achievable.
The 5 Strategies That Actually Work
1. Post-Meal Movement
Walking after meals is the most time-efficient blood sugar intervention available without medication. A 10-minute walk taken within 30 minutes of eating reduces post-meal glucose by significantly more than a single 30-minute walk taken at a different time of day. The mechanism is direct: muscle contractions during walking activate GLUT4 glucose transporters through an insulin-independent pathway, pulling glucose out of the bloodstream and into cells.
You do not need to walk far or fast. A gentle 10-minute walk after each main meal produces measurable glycemic benefits. For the full evidence on timing and intensity: read our guide to walking after meals for blood sugar.
2. Dietary Changes That Matter
The most evidence-supported dietary changes for prediabetes are not complicated: reduce refined carbohydrates and ultra-processed foods, increase fiber, and control portion sizes at meals. No single diet has been proven superior — the DPP used a low-fat approach, while Mediterranean and low-carbohydrate patterns also show strong results in clinical trials. The common thread is replacing processed carbohydrates with whole foods, vegetables, and quality protein.
Specific changes that consistently reduce A1C and fasting glucose:
- Replace white rice, white bread, and refined cereals with non-starchy vegetables, legumes, or whole grains
- Prioritize protein at breakfast to reduce morning glucose spikes
- Eat fiber before carbohydrates at meals (salad before rice, vegetables before pasta)
- Eliminate sugar-sweetened beverages — liquid glucose produces the sharpest spikes
For a complete breakdown of what to eat and what to avoid, including specific food swaps: read our prediabetes diet guide. For breakfast specifically — the highest-leverage meal for blood sugar: read our guide to the best breakfast for prediabetes.
3. Weight Loss (Even Small Amounts)
The DPP goal was 7% body weight loss — about 10 to 15 pounds for most participants. At that level, visceral fat decreases, insulin receptor sensitivity measurably improves, and the pancreas reduces its compensatory insulin output. Greater weight loss produces proportionally greater benefit, but even 5% weight reduction produces clinically meaningful improvement in insulin sensitivity.
Importantly, weight loss is not required for reversal in people who are not overweight. Prediabetes occurs in people at all body weights, and lifestyle improvements work regardless of whether significant weight loss occurs. For a direct look at this: read our guide on reversing prediabetes without weight loss.
4. Sleep and Stress Management
Sleep deprivation and chronic stress are metabolic stressors that raise blood glucose independently of diet and exercise. Cortisol triggers the liver to release stored glucose (gluconeogenesis), and this happens regardless of what you ate. Addressing sleep quality and stress is not optional in a complete prediabetes strategy — it is foundational. Improving sleep alone, without dietary changes, has been shown to meaningfully improve insulin sensitivity in sleep-deprived adults.
5. Evidence-Based Supplements (As Add-Ons)
Supplements do not replace lifestyle changes, but specific ones have meaningful clinical evidence as additions to an already-working lifestyle strategy. Berberine has the strongest evidence — a 2023 umbrella meta-analysis found it reduces A1C by an average of 0.45 percentage points and fasting glucose by 10.6 mg/dL, with efficacy comparable to low-dose metformin. Vitamin D supplementation (when deficient) and cinnamon also show consistent effects in meta-analyses of multiple randomized trials.
For the complete evidence breakdown across all major supplements: read our guide to the best supplements for prediabetes.
How Long Does Reversal Take?
A1C reflects the average blood sugar over the past 90 days, so the earliest you can meaningfully measure progress from a new intervention is 3 months. Most people who implement the strategies above consistently see measurable A1C improvement at the 3-month mark, and return to normal range (below 5.7%) within 6 to 12 months.
Fasting glucose responds faster — changes are sometimes visible within 4 to 6 weeks of consistent dietary and exercise changes. If you have access to a home glucose monitor, tracking fasting glucose gives earlier feedback on whether an intervention is working before your next A1C test.
The most important variable is consistency, not intensity. Aggressive short-term efforts followed by return to old habits do not produce lasting reversal. The DPP lifestyle group made moderate, sustainable changes — and those changes produced durable results that persisted at 10-year follow-up.
What to Do Right After Diagnosis
If you were recently diagnosed, the practical first steps are:
- Get your baseline numbers. Ask your doctor for your specific A1C percentage and fasting glucose result. Know exactly where you are in the prediabetes range — it matters for tracking progress.
- Schedule a follow-up. A1C retest in 3 months gives you the first data point on whether your interventions are working.
- Start with post-meal walks. Ten minutes after each main meal is the lowest barrier, highest-impact starting point for most people.
- Remove one high-glycemic staple. Identify the one food that contributes most to your blood sugar load (often a sugary drink, white bread, or refined cereal) and replace it first.
- Ask your doctor the right questions. Not all doctors proactively discuss reversal. Specific questions get better answers. For exactly what to ask: read our guide to questions to ask your doctor after a prediabetes diagnosis.
For a structured 30-day action plan starting from diagnosis: read our 30-day prediabetes plan for the newly diagnosed.
Frequently Asked Questions
Can prediabetes be reversed naturally?
Yes. The Diabetes Prevention Program — the largest prediabetes study ever conducted — found that lifestyle intervention (150 minutes of weekly exercise and modest dietary changes) reduced progression to type 2 diabetes by 58% over three years. Returning A1C below 5.7% and fasting glucose below 100 mg/dL through lifestyle changes alone is achievable for most people with prediabetes.
What A1C level is considered prediabetes?
According to the American Diabetes Association 2025 Standards of Care, prediabetes is defined as an A1C between 5.7% and 6.4%. Below 5.7% is normal. At 6.5% or above, a type 2 diabetes diagnosis is made. Fasting plasma glucose between 100 and 125 mg/dL also meets the prediabetes criteria.
How long does it take to reverse prediabetes?
Most people who implement consistent lifestyle changes see measurable A1C improvement at their 3-month retest, and return to normal range within 6 to 12 months. A1C reflects 90 days of average blood sugar, so early testing will not capture recent changes. Fasting glucose tends to respond faster — sometimes within 4 to 6 weeks of dietary and exercise changes.
What foods should I avoid with prediabetes?
The highest-impact foods to reduce or eliminate with prediabetes are sugar-sweetened beverages (soda, juice, sweetened coffee drinks), white bread and refined flour products, white rice, breakfast cereals with added sugar, and ultra-processed snack foods. These produce rapid blood glucose spikes that drive insulin resistance over time. Replacing them with vegetables, legumes, whole grains, and quality protein produces the most consistent glycemic improvement.
Is prediabetes serious?
Prediabetes is a serious metabolic condition that increases the risk of type 2 diabetes, cardiovascular disease, and kidney disease. Without intervention, 15 to 30% of people with prediabetes develop type 2 diabetes within 5 years. However, it is also the most reversible stage of metabolic dysfunction — the evidence for lifestyle-based reversal at the prediabetes stage is substantially stronger than at the type 2 diabetes stage.
Do I need medication for prediabetes?
Medication is not required for most people with prediabetes. The Diabetes Prevention Program found that lifestyle intervention outperformed metformin (58% vs. 31% reduction in diabetes progression). The ADA guidelines recommend lifestyle intervention as the first-line approach for prediabetes, with metformin considered for high-risk individuals (A1C close to 6.4%, BMI above 35, or history of gestational diabetes). Discuss your specific risk level with your doctor.
Sources: Knowler WC et al., Diabetes Prevention Program (NEJM, 2002). Tuomilehto J et al., Finnish Diabetes Prevention Study (NEJM, 2001). American Diabetes Association Standards of Care 2025. CDC National Diabetes Statistics Report 2023. PubMed 38016844, berberine umbrella meta-analysis (Clinical Therapeutics, 2023). Colberg SR et al., ADA/ACSM joint position statement on exercise and type 2 diabetes.
Adults over 50 experience prediabetes symptoms differently than younger patients. For age-specific warning signs, see Prediabetes Symptoms in Adults Over 50.


